Early gynecologic cancers, especially high-grade serous carcinoma, can be very difficult to detect. These cancers may be extremely small and limited to only a tiny part of the fallopian tube, making them easy to miss with routine tissue sampling.
The SEE-FIM protocol (Sectioning and Extensively Examining the FIMbria) was developed to help solve this problem. It improves cancer detection by increasing both how much tissue is examined and how carefully high-risk areas are sampled.
Any pathologists’ assistant working in a lab that handles gynecologic cancer specimens will likely encounter this protocol. Understanding how and why SEE-FIM is used is important for accurate specimen processing and diagnosis.
By standardizing fallopian tube sampling and focusing on the areas most likely to contain early cancer, the SEE-FIM protocol greatly improves diagnostic accuracy for fallopian tube and ovarian tissues.
Why the SEE-FIM Protocol Matters
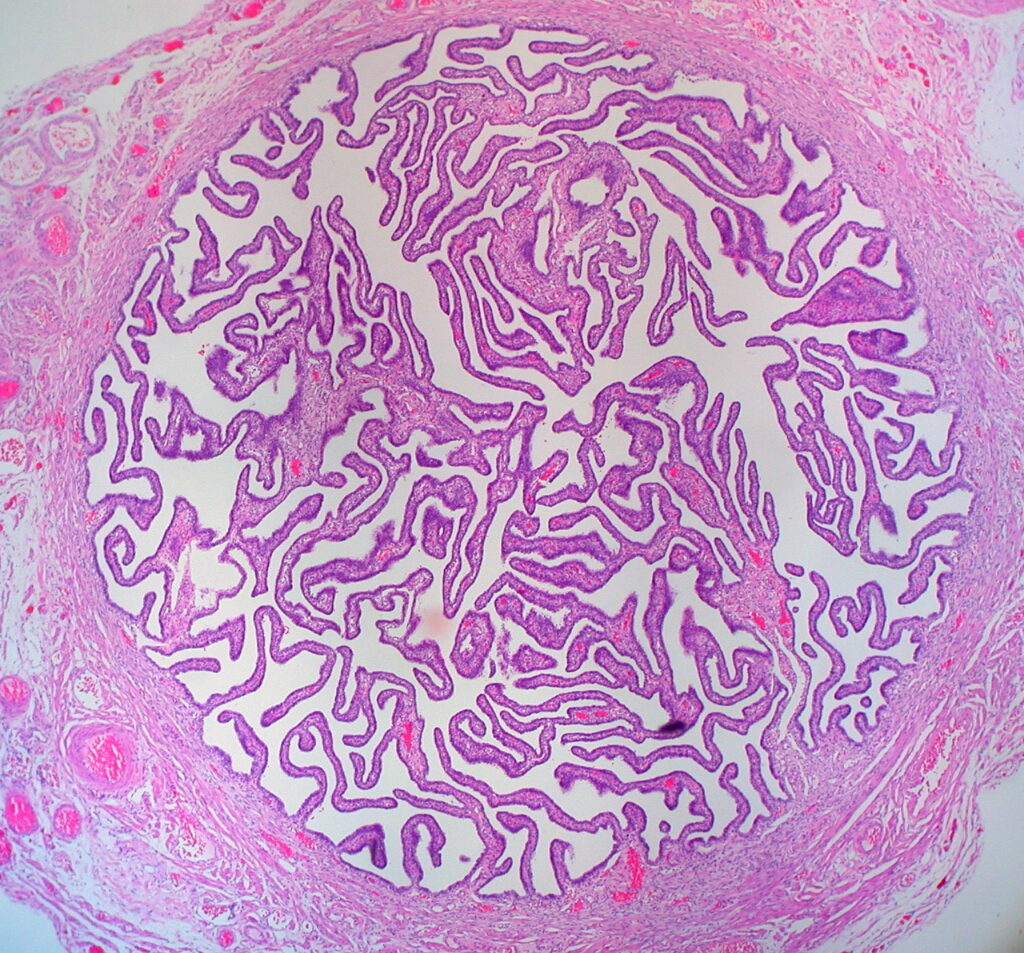
Traditional fallopian tube sampling usually uses only a few cross-sections taken from different parts of the tube. While this works for many non-cancerous conditions, it can miss very small cancers that affect only a tiny area of the lining.
Rather than checking just a few small sections, the SEE-FIM protocol closely examines a larger amount of tissue. It pays special attention to the fimbriated end because many cancers once thought to start in the ovary actually begin there.
Extensive Examination of the Fimbria
One of the main features of the SEE-FIM protocol is its strong focus on the fimbrial end of the fallopian tube. This part of the tube is examined much more closely than in standard sampling.
Targeting High-Risk Anatomy
The fimbria is an area where early cancer is more likely to develop, especially in patients with inherited cancer risks such as BRCA mutations. Many cancers that were once believed to start in the ovary are now known to begin in the far end of the fallopian tube.
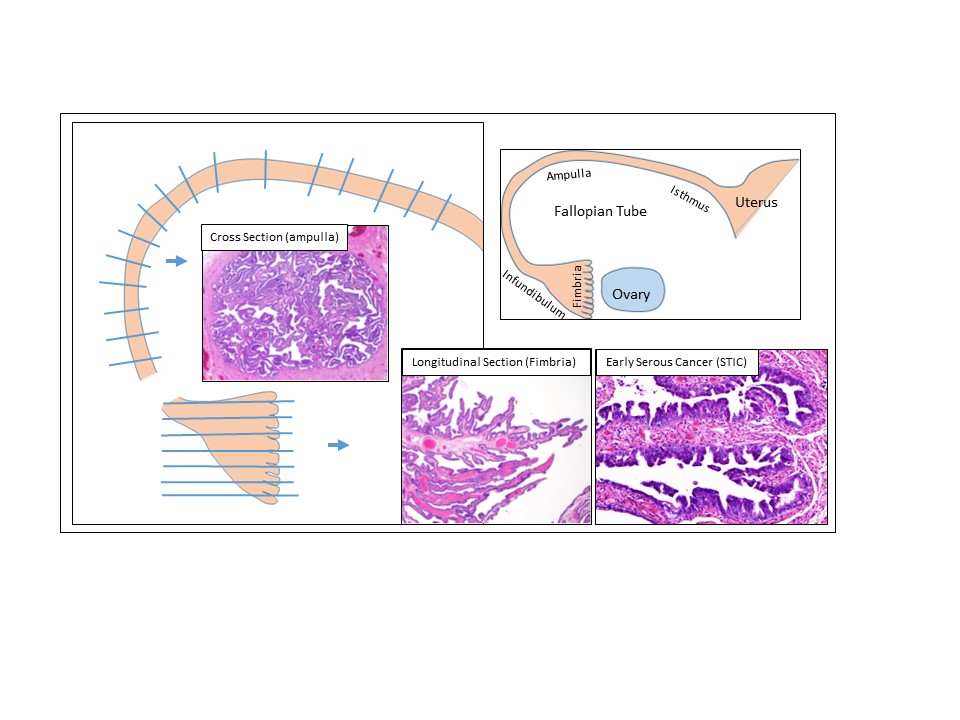
Longitudinal Sectioning Technique
Instead of cutting the tube into random cross-sections, the last 2 cm of the tube is removed, opened lengthwise, and laid flat. This makes it easier to see the full surface of the fimbria lining under the microscope.
Maximizing Surface Area Examined
Cutting the fimbria lengthwise greatly increases how much of the lining can be examined. This makes it easier to find very small or early cancers, such as serous tubal intraepithelial carcinoma (STIC), which may involve only a tiny number of cells.
Complete Submission of the Fimbria
All sections from the fimbriated end are submitted for examination. This ensures that the most important part of the tube is fully reviewed and not partially missed.
Comprehensive Sampling of the Entire Tube
For patients with higher cancer risk, the SEE-FIM protocol does not stop at the fimbria. In these cases, the entire rest of the fallopian tube is also examined.
Who Requires Full Tubal Submission?
Full examination of the tube is usually required for patients who:
- Have BRCA1 or BRCA2 mutations
- Have known or suspected high-grade serous carcinoma
- Are undergoing preventative surgery to reduce cancer risk
- Have fallopian tubes that look abnormal on gross examination
Serial Sectioning of the Remaining Tube
In these patients, the entire length of the remaining tube is cut into cross-sections spaced about 2–3 mm apart. This allows careful review of the whole tube.
Total Tissue Examination
All of these sections are submitted for microscopic review. Examining the entire tube like this reduces the chance of missing small or scattered cancerous areas.
Risk-Stratified Approaches: Modified vs Full SEE-FIM
To balance accuracy with lab workload, the SEE-FIM protocol is used differently depending on patient risk.
Modified SEE-FIM
The modified SEE-FIM approach is used for patients who:
- Have no known genetic risk
- Have no history of high-grade serous carcinoma
- Have fallopian tubes that look normal
This approach includes:
- Full longitudinal submission of the fimbria
- One representative cross-section from the middle of the remaining tube
Depending on section size, it is often possible to fit two cross-sections into one cassette. This can improve detection without increasing workload.
Full SEE-FIM
The full SEE-FIM protocol is used for patients who:
- Have a known genetic or clinical cancer risk
- Have abnormal-appearing tubes
This approach includes:
- Full longitudinal submission of the fimbria
- Serial cross-sections of the entire remaining tube, all submitted for review
Why Diagnostic Accuracy Improves
The SEE-FIM protocol improves diagnostic accuracy in two main ways:
- More Tissue Is Examined
When more tissue is looked at under the microscope, there are fewer places for small cancers to hide. - Focus on the Highest-Risk Area
By concentrating on the fimbria, the protocol focuses on the part of the tube where early cancer is most likely to be found.