When grossing bowel specimens, one of the most important margins is the radial margin. Understanding this margin is crucial for identifying it and grossing these specimens properly.
The Basic Concept
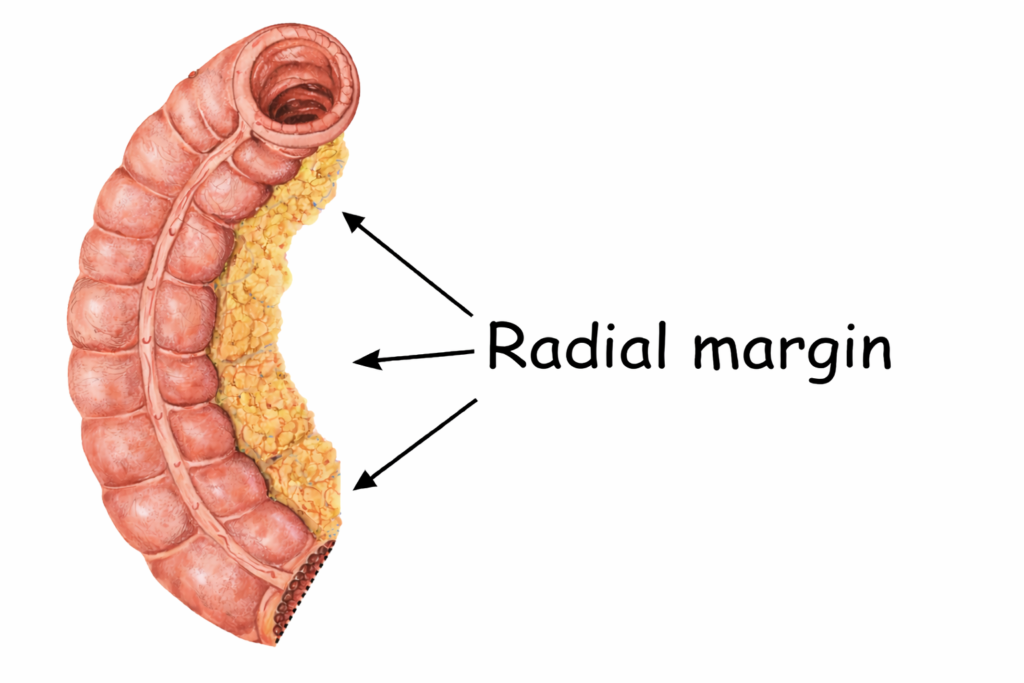
The radial margin refers to the non-peritonealized surface created when the surgeon dissects the bowel away from surrounding tissues. It represents the adventitial soft tissue margin of bowel resections.
It is not the same as the proximal or distal margin.
The radial margin is created when the surgeon cuts through the pericolic fat to remove the segment of colon. This fat contains blood vessels and lymphatic channels that normally supply and drain the bowel. Cutting through this tissue separates those structures from the portion of colon being removed.
Why the Radial Margin Matters
The radial margin is critically important because:
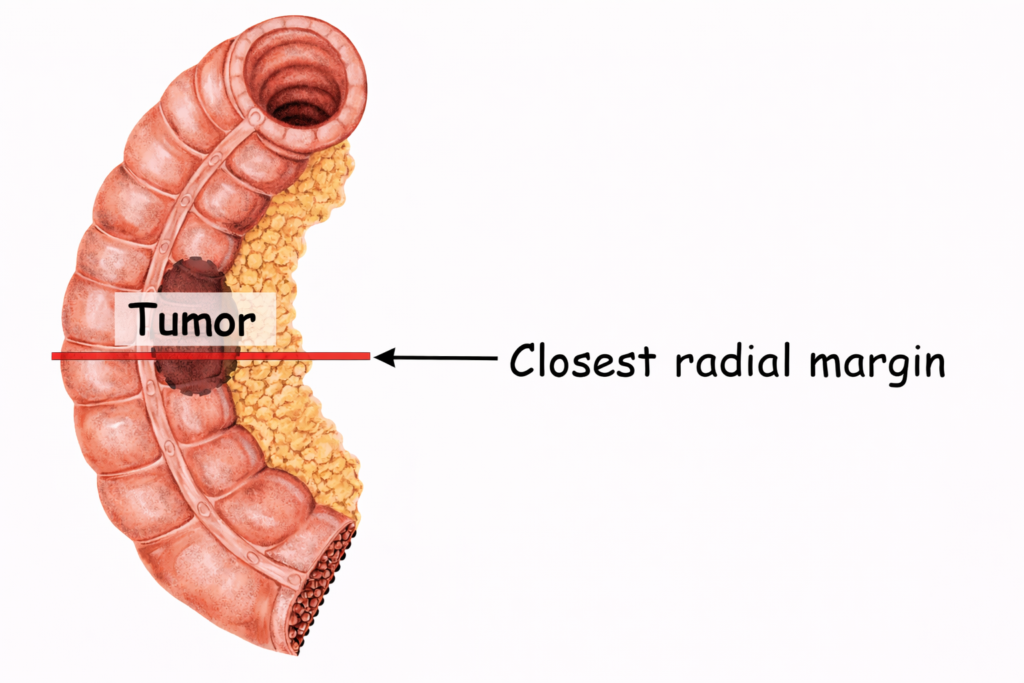
- If a tumor is close to this surface, it may indicate more aggressive disease or a greater likelihood of recurrence
- Tumor involvement of the radial margin is the most critical factor in predicting local recurrence (particularly in rectal cancer). A positive radial margin in rectal cancer increases the risk of recurrence by 3.5-fold and doubles the risk of death from disease.
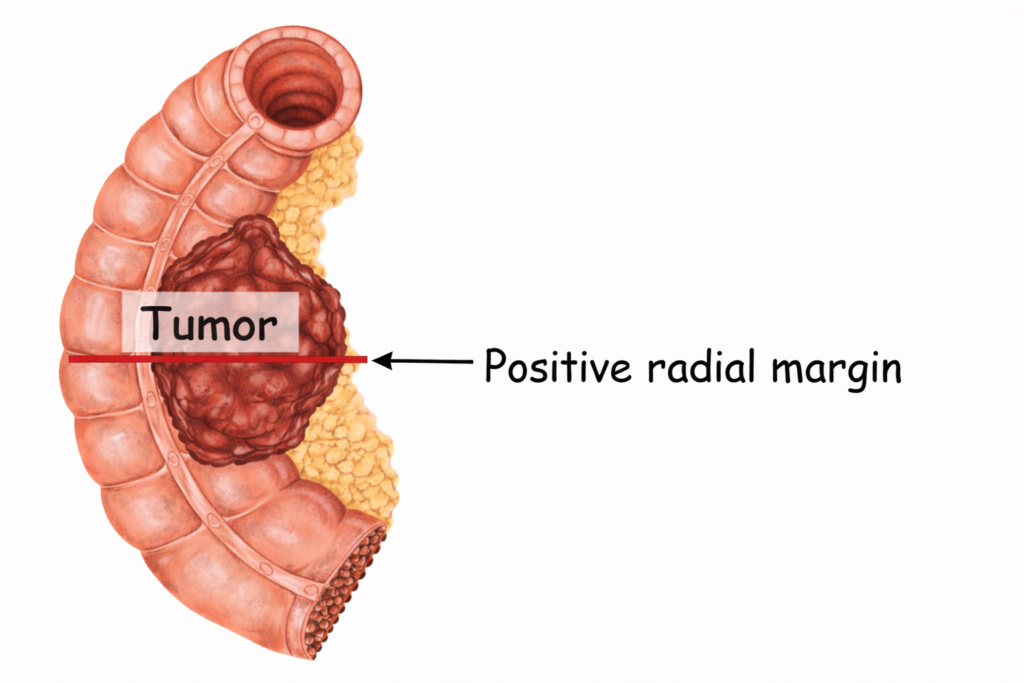
- The area where the tumor comes closest to the radial margin is important because it represents the most likely route for cancer cells to escape the primary tumor and spread. If tumor cells are present right at the radial margin, this means the tumor was cut through at that point. In other words, cancer has been left behind in the patient, resulting in a positive radial margin. If not treated, these residual tumor cells can continue to grow and potentially spread.
How to Identify the Radial Margin
If unsure how to identify the radial margin when handling a specimen, focus on these principles:
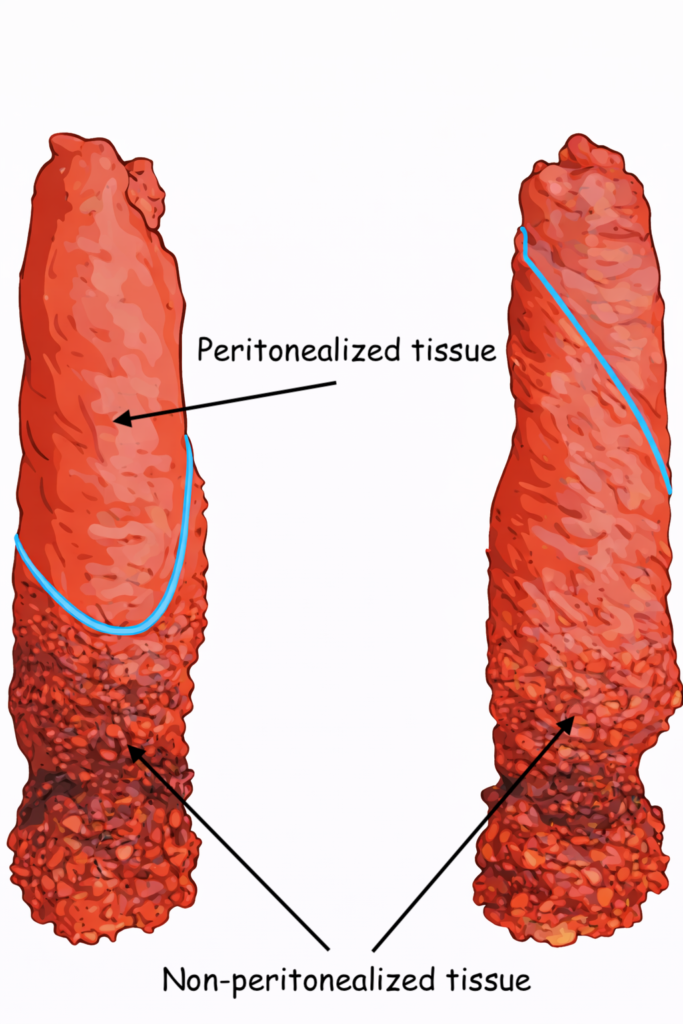
- Peritonealized surfaces
These are smooth, shiny, and represent areas freely exposed to the abdominal cavity. This is not a margin. - Non-peritonealized surfaces
These appear duller, are roughened and may only involve part of the bowel circumference depending on the segment resected. This represents surfaces directly against retroperitoneal fat/surfaces that are not free in the peritoneal cavity. You may recognize a line of cautery from the surgery at the transition from peritonealized to non-peritonealized tissue.- The radial margin
This is the non-peritonealized surface where the surgeon created a dissection plane, either through sharp or blunt dissection (this is why you can often recognize a line of cautery).
- The radial margin
Radial margin in a low anterior resection specimen
Radial margin vs mesenteric margin – are they the same thing?
- In colon cancer, the relevant non-peritonealized soft tissue margin is called the radial margin
- In small bowel resections, a similar concept exists but is typically referred to as the mesenteric margin
- The key unifying idea is:
- It’s a surgically created soft tissue margin
- Not a mucosal margin
- Often the closest margin in deeply invasive tumors
Common Pitfalls
- Struggling to identify peritonealized vs non-peritonealized tissue → aka where the radial margin actually is
- Just because the tumor extends into the fat does not mean the radial margin is positive
- Tumor extension to the serosa is not the same as a positive radial margin.
- Assuming all colon is fully peritonealized. It isn’t, especially as you move distally toward the rectum. In these cases, tumor that would represent serosal involvement in a more proximal segment of bowel may actually be extending to non-peritonealized tissue and therefore represent a positive radial margin.